Akioka N, Kashiwazaki D, Koh M, Kuwayama N, Tanaka K, Kuroda S.
Comprehensive Hybrid Strategy for Carotid Artery Stenosis with 8 Rules “Toyama Carotid 8”
No Shinkei Geka. 2016 Jan;44(1):31-8.
Abstract:
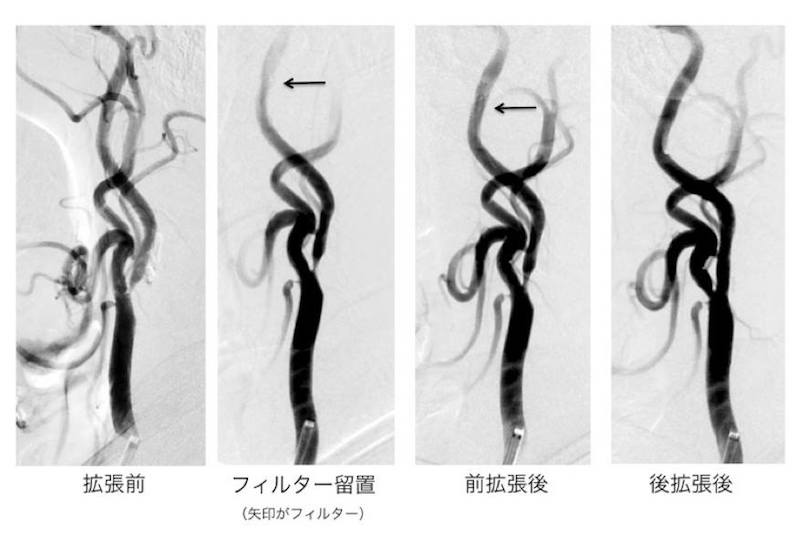
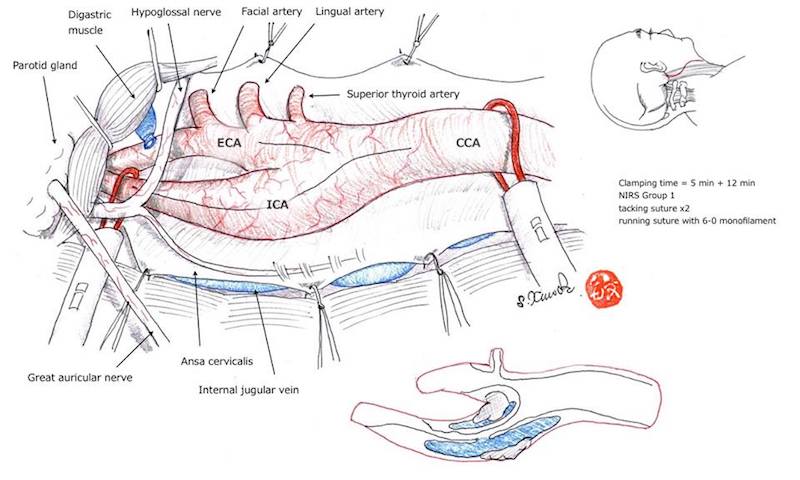
In this paper, the preliminary results of carotid endarterectomy(CEA)and carotid artery stenting(CAS)for patients with carotid artery stenosis based on the 8 Rules “Toyama Carotid 8” are reported. This study included 104 patients who underwent CEA or CAS for carotid artery stenosis between March 2012 and January 2015. Toyama 8 Rules primarily recommend CEA and CAS for symptomatic and asymptomatic lesions, respectively. However, crossover of therapeutic options can be performed in patients at high surgical risk associated with CEA or CAS. Monitoring of platelet function is important prior to CAS. Internal shunting and near infrared spectroscopy monitoring are essential in CEA. Temporary cardiac pacing is essential in CAS. The choice of protection device and stent depends on the results of MR plaque imaging. Cerebral blood flow measurement is mandatory before and after CEA/CAS. Fifty-two CEAs and 52 CASs were performed for 55 symptomatic and 49 asymptomatic lesions. Crossover of therapeutic options was performed in 10(18%)of 55 symptomatic lesions and 7(14%)of 49 asymptomatic lesions. The 30-day morbidity rate was 1.9% in CEA and 1.9% in CAS. Postoperative diffusion-weighted magnetic resonance imaging showed fresh ischemic lesions in 5 patients who underwent CEA(10%)and 9 who underwent CAS(17%). Hyperperfusion syndrome occurred in one patient(1.0%). A management protocol for carotid artery stenosis needs to be established in hospitals to allow sharing of information and improvement in the short-term results of CEA / CAS for carotid artery stenosis. Further studies are warranted to evaluate the long-term outcome.